企业邮箱
企业邮箱





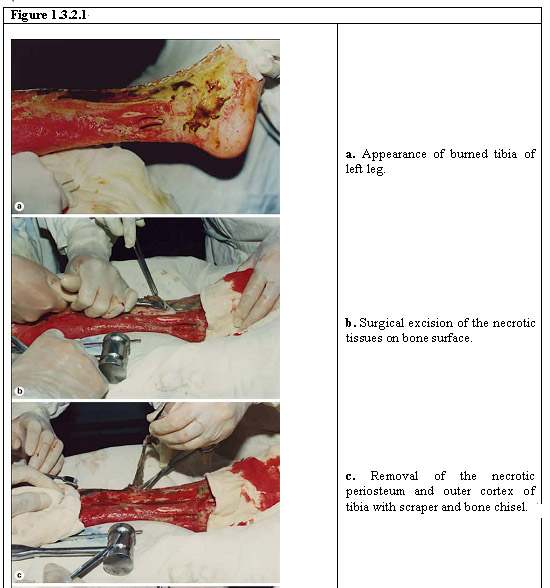
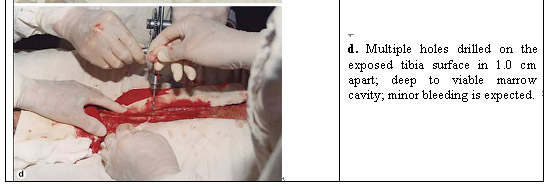
When the burn destroys the skin and underlying tissue to reach the bone, the injury can result in compartment syndrome and threaten the patient’s life or limb.
Dr. Xu led a pioneering work in the regeneration of tissues beyond the skin by utilizing bone marrow cells exuding from holes drilled on the bone.
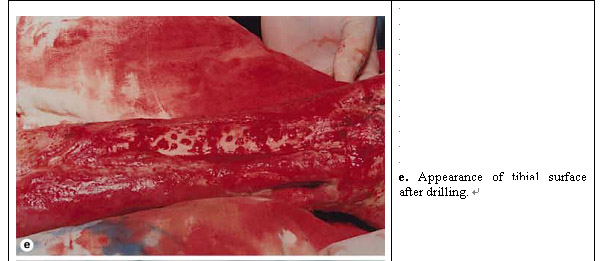
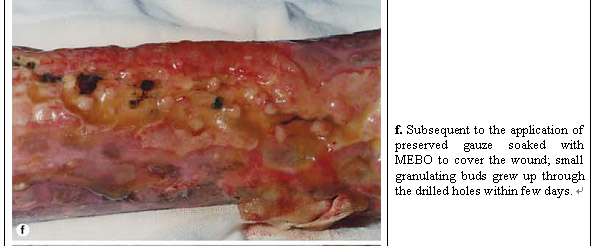
As shown in Figure 1.3.2.1, the patient’s left leg had burn wounds with tibia exposed and was treated with MEBT/MEBO. Multiple holes were drilled in the exposed tibia and covered with gauzed soaked with MEBO wound ointment. Granulation tissue developed from the bone marrow cells migrated from the cavities created and under the regenerative condition provided by MEBT/MEBO the bone marrow cells were converted to multiple different cell types needed for regeneration of muscle, tendon, ligament and other soft tissue.
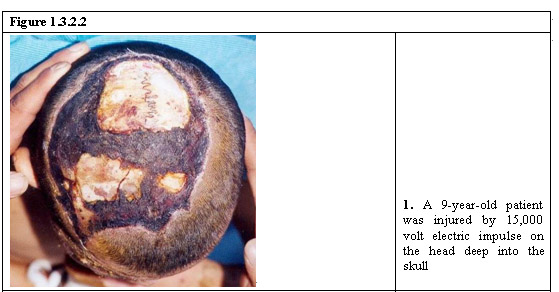
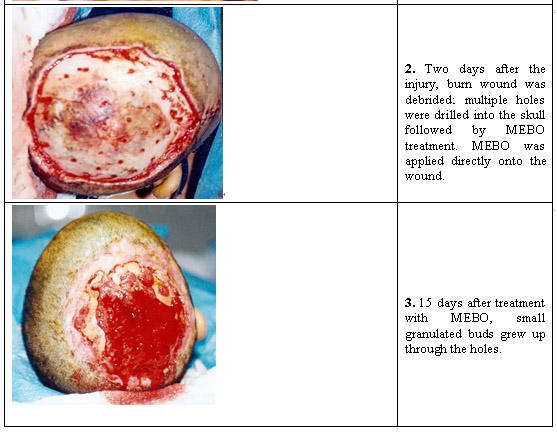
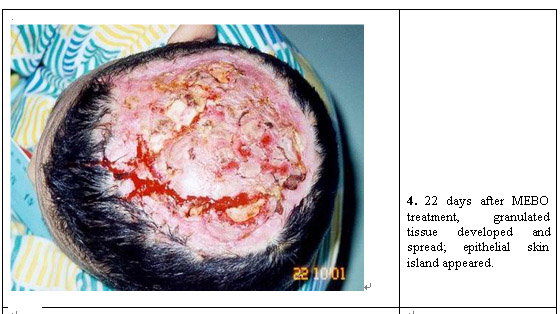
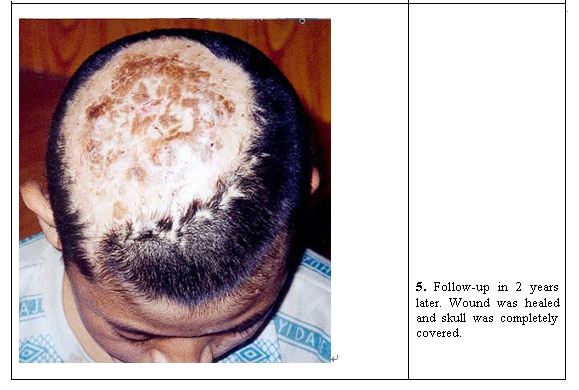
Shown in Figure 1.3.2.2 is another case where a 9 year-old patient’s head was injured by high-voltage electric burn and the injury reached deep into the skull. He was treated with MEBT/MEBO. Multiple holes were drilled on the skull to allow cultivation and conversion of bone marrow cells in order to regeneration soft tissue and the skin on his head. As shown below, 2 years after the injury his skull was completely covered with regenerated tissue and skin.

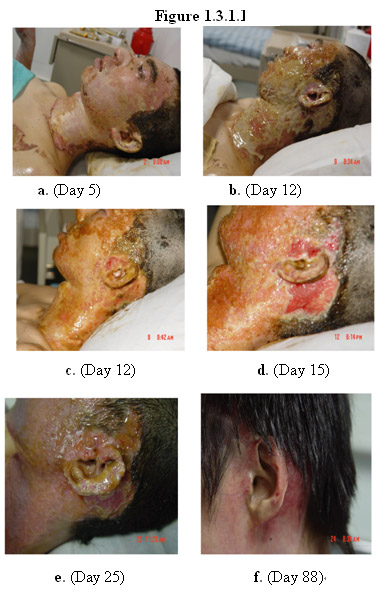
MEBT/MEBO has also been used to successful regenerate the skin and underlying soft tissue of the ear after burn injury. The exposed and projecting auricular conchas are easy to be injured. The skin and subcutaneous tissue of external ear are thin, so ear burn always compromises auricular cartilage. Besides, since it was near hair and was connected with external auditory canals, and ears themselves were too irregular and rough to be cleaned, ear burn was usually complicated with infections and suppurative perichondritis of auricle post injury.
Shown in Figure 1.3.1.1 is a case where the patient was burned in face and neck by boiling oil. As shown below, on day 88 since the burn injury the structure and function of his ear was substantially restored with no compromise of hearing.
Shown in Figure 1.3.1.2 is the same case shown in Figure 1.2.4.1 where the patient’s ear also sustained deep burn injury and treated with MEBT/MEBO. As shown below, on day 30 post burn injury his wounds on his face, neck substantially healed. A follow up examination 3 months later revealed that the structure and function of his ear was substantially restored with no compromise of hearing (Figure 1.3.1.2j).


4.1 Regeneration of Soft Tissue
MEBT/MEBO has also been used to successful regenerate the skin and underlying soft tissue of the ear after burn injury. The exposed and projecting auricular conchas are easy to be injured. The skin and subcutaneous tissue of external ear are thin, so ear burn always compromises auricular cartilage. Besides, since it was near hair and was connected with external auditory canals, and ears themselves were too irregular and rough to be cleaned, ear burn was usually complicated with infections and suppurative perichondritis of auricle post injury.
Shown in Figure 1.3.1.1 is a case where the patient was burned in face and neck by boiling oil. As shown below, on day 88 since the burn injury the structure and function of his ear was substantially restored with no compromise of hearing.
Shown in Figure 1.3.1.2 is the same case shown in Figure 1.2.4.1 where the patient’s ear also sustained deep burn injury and treated with MEBT/MEBO. As shown below, on day 30 post burn injury his wounds on his face, neck substantially healed. A follow up examination 3 months later revealed that the structure and function of his ear was substantially restored with no compromise of hearing (Figure 1.3.1.2j).
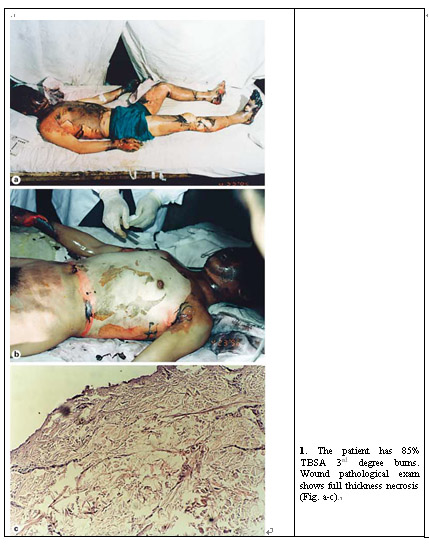
Case 1: Male, age 18, burned by gas flames, 95% TBSA (superficial 2nd degree burn 30%, deep 2nd degree burn 59%, 3rd degree burn 6%), treated with MEBT/MEBO for 55 days.
Case 2: Male, age 21, scalded by hot water, 98% TBSA (superficial 2nd degree burn 40%, deep 2nd degree burn 58%), treated with MEBT/MEBO for 30 days.
Case 3: Female, age 20, burned by gas flames, 91% TBSA (superficial 2nd degree burn 10%, deep 2nd degree burn 76%, 3rd degree burn 5%), treated with MEBT/MEBO for 52 days.

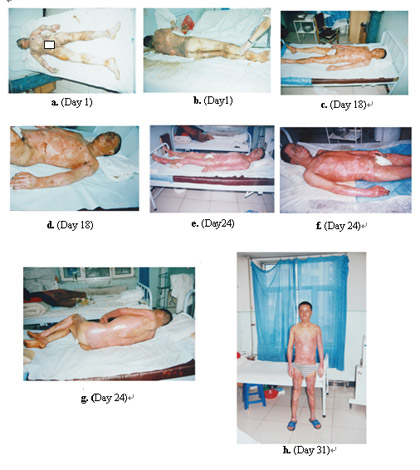
Case 5: Male, age 31, burned by nitre flames, 90% TBSA (deep 2nd degree burn 60%, superficial 3rd degree burn 20%, deep 3rd degree burn 10%), treated with MEBT/MEBO for 31 days.
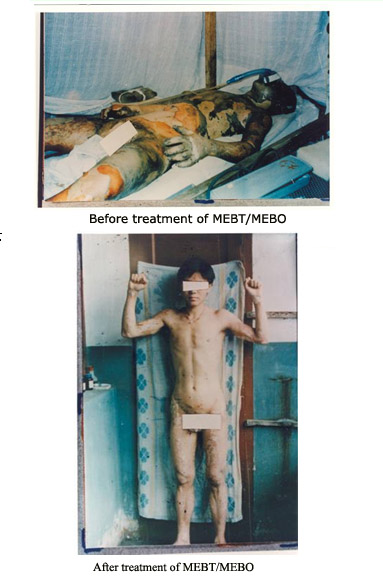
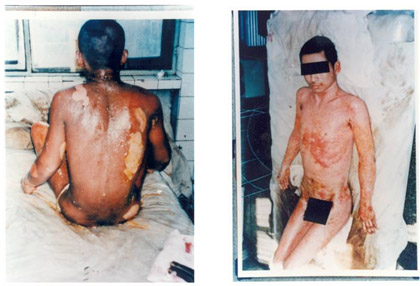
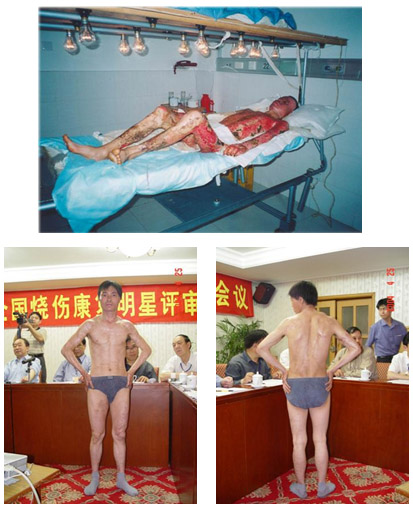
Extremely large (>40% TBSA) and deep (>2nd degree) burn wounds pose a major medical challenge due to massive loss of tissue and potential systemic complications. To save life and heal the wounds, aggressive surgical approaches with early tangential excision and wound closure are usually taken. Autografts from uninjured skin of the patient are taken to be used to cover the burn wounds, the wounds as a result of which further increase the TBSA affected. When the patient’s skin donor sites are limited or the overall patient condition do not permit immediate grafting with autologous skin, human cadaver allograft skin (HCAS) and xenografts are used as temporary burn wound cover. Serious problems, however, are associated with HCSA and xenografts, including limited supply, variable and occasionally poor quality, inconvenience of harvesting skin in the mortuary, and ultimate immune rejection. Cultured epithelial autografts have been developed for the treatment of extensively deep burns. A major disadvantage of this approach is the delay in providing cultured keratinocyte sheets for practical clinical use, in addition to fragility and difficult handling of the grafts, an unpredictable “take” and extremely high costs. Widespread use of cultured autografts has been primarily hampered by poor long-term clinical results. Even if the patient’s life is saved, severe disfigurement and disablement often result.
Against this grim background, the innovative approach taken by Dr. Xu represents a major paradigm shift. By using MEBT/MEBO, Dr. Xu and now a network of clinicians throughout China have successfully treated tens of thousands of patients with deep, extensive burn wounds. The patients not only survived, but also thrived with minimum disfigurement and disablement.
Shown below are a few examples of patients treated with MEBT/MEBO.
Figure 1.2.5.1 Partial-Thickness Burns Treated with MEBT/MEBO
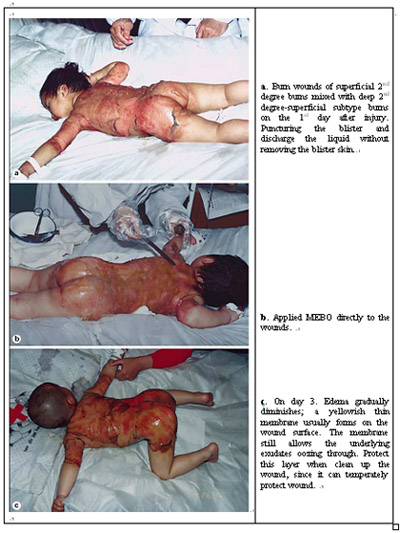
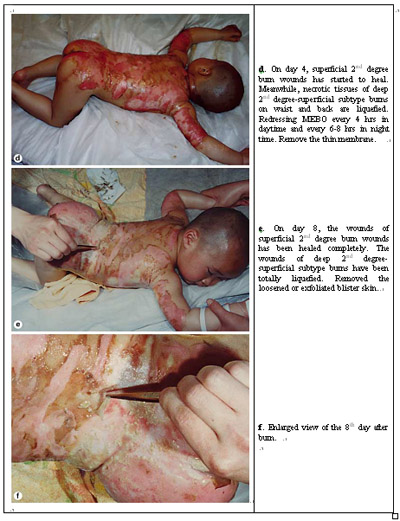
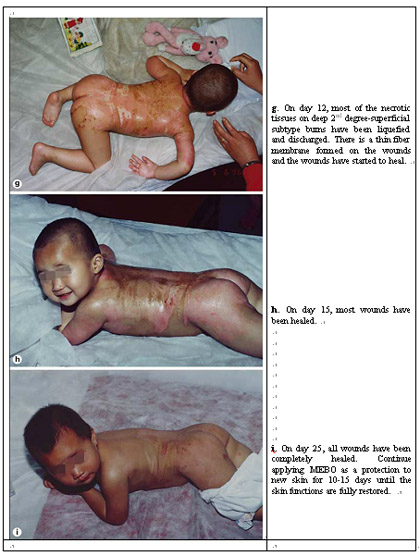
Figure 1.2.5.2 Treatment of Deep 3rd Degree Burns with MEBT/MEBO

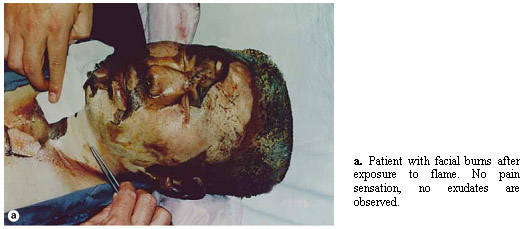
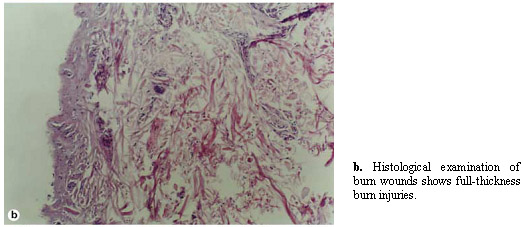
The face constitutes 5-10% of the body’s surface area, varying according to age. Face burns cause a considerable loss of fluids owing to the elasticity of the tissues affected and the abundance of vascular tissue. In deep partial-thickness burns, spontaneous recovery occurs with the formation of a considerable quantity of unaesthetic scarring. Third-degree burns (full-thickness burns) destroy both the epidermis and the entire dermis and are insensate because of the loss of sensory nerve endings. A full-thickness burn is dry and leathery with a gray, white, or translucent color; it turns brown or black in color, characteristic of an eschar. Most of these wounds do not heal spontaneously unless they are very small, skin grafting is often needed for closing the wounds, and the resulting scars may be quite disfiguring, which necessitates post-healing reconstructive surgery on the scars.
MEBT/MEBO has been used in thousands of cases to successfully treat deep facial burns with minimum scarring and disfigurement, thereby obviating the need for post-healing reconstructive surgery.
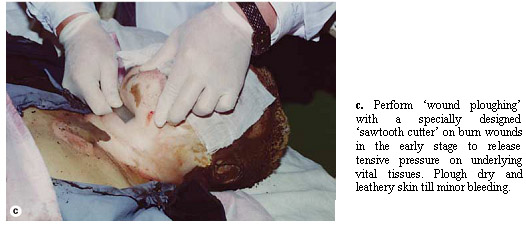
Shown in Figure 1.2.4.1 is an example of using MEBT/MEBO to treat a patient with full-thickness burns on his face and neck.
Figure 1.2.4.1






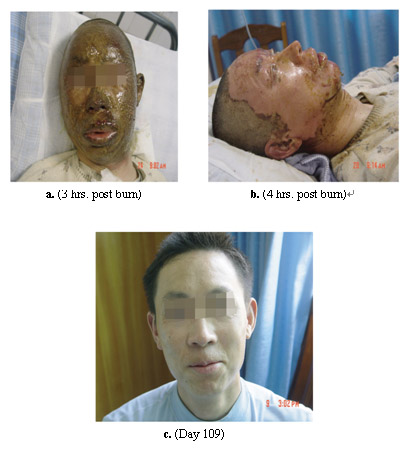
Shown in Figure 1.2.4.2 is another example of treatment of deep facial burn wounds using MEBT/MEBO.
This patient’s face was burned by electric arc, resulting in superficial 2nd degree and superficial 3rd degree burns. As shown below, on day 109 since the treatment with MEBT/MEBO, the skin on his face was regenerated with no apparent scarring and loss of function.
Deep 2nd and 3rd degree burns on the hand assume a high priority from the onset of care in order to preserve its sensory and mobile functions. As shown in Figure 1.0.2 severe burn injury of the hand can lead to severe joint contracture and loss of hand function. Normally, early excision and sheet autograft closure are recommended. Hand therapy is continued throughout the healing period, halted only in the few days immediately after grafting. Sometimes only suboptimal function can be obtained in a long term.
MEBT/MEBO has been used to successfully treat deep, severe hand burns without skin grafting and with satisfactory restoration of form and function to the injured hand.
Shown in Figure 1.2.3.1 is an example of using MEBT/MEBO to treat deep 2nd degree burn of a hand of a patient.
Figure 1.2.3.1


As described in detail by Xu in “Clinical Procedure and Histological Observation of Full-Thickness Burns Treated with MEBO” in Burns Regenerative Medicine and Therapy, 1st ed., Basel: Karger; 2004. p. 111-114, MEBT/MEBO was used to treat a patient with extensive full-thickness burns in her lower extremities.
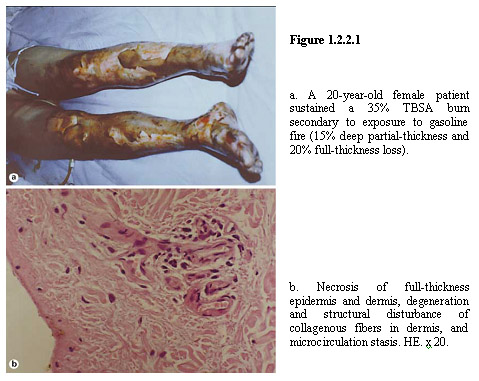
A 20-year-old female patient was hospitalized at 12 h after a gasoline fire burn and was diagnosed with 35% TBSA burn (15% deep partial-thickness and 20% full-thickness burns on both lower extremities). The epidermis was necrotic and detached and the dermal layer was degenerated and necrotic with a waxy yellow and waxy white appearance (Figure 1.2.2.1a). The pathological section examination of the sampled local wound tissues revealed a necrosis in full-thickness of epidermis and dermis, degeneration and structural disturbance of collagenous fibers in dermis, and microcirculation stasis (Figure 1.2.2.1b).
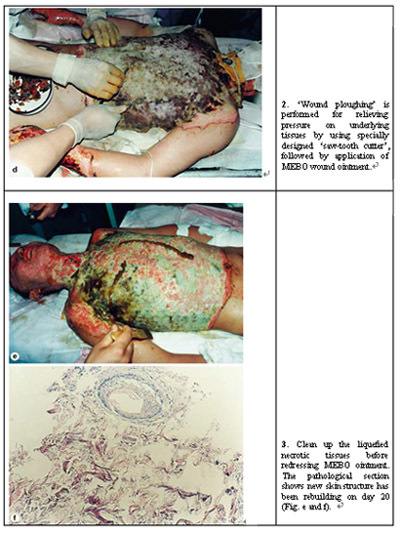
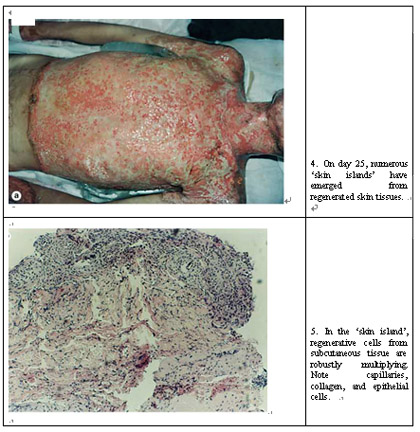
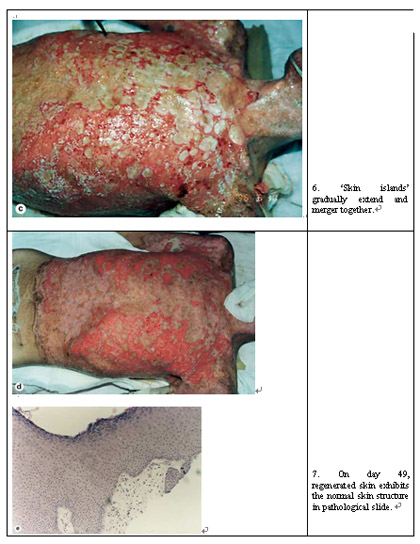
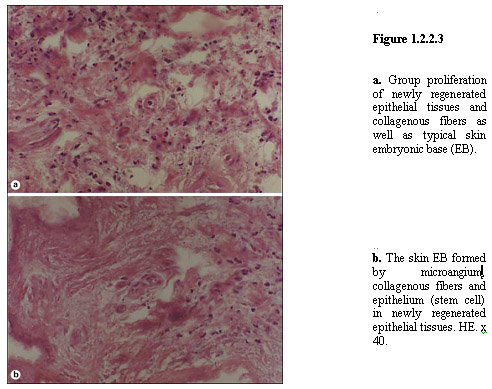
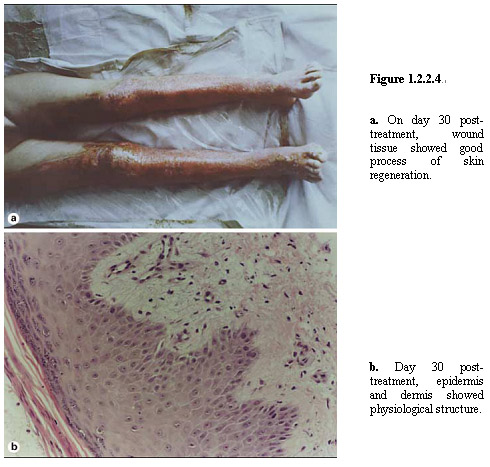
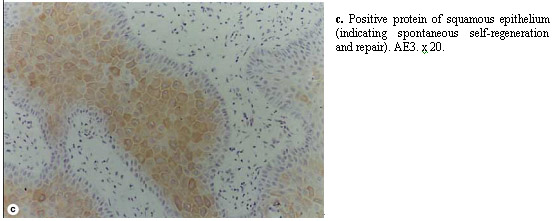
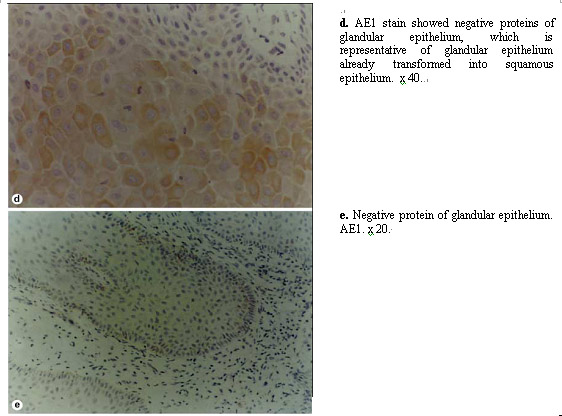
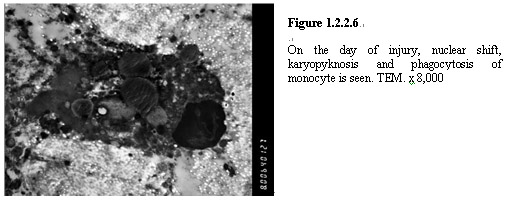
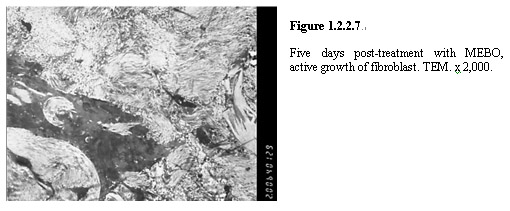
After admission, the patient was treated with MEBT/MEBO wound ointment to protect burn tissue. At 48 h postburn, the wounds began to liquefy and the liquefaction was complete by day 4 (Figure 1.2.2.2). The liquefied products were gently removed from the wound surface before MEBO ointment was reapplied every 3-4 h. Repeat biopsy at the same burned location was performed for pathological examination. The results showed massive granulation tissues among the necrotic epithelial tissue, a proliferation of newly regenerated epithelial cells with collagenous fibers, as well as the typical skin embryonic base (EB) (Figure 1.2.2.3a, b). After a 10-day application of MEBO ointment, embryonic-like epithelial tissues were observed in epithelial tissues sampled from the wound edge. At 20 days post-treatment with MEBO, the pathological examination of deep burns wounds tissue showed the presence of the newly formed intact stratified squamous epithelium. The epithelial cells of the superficial layer appeared normal. Appearance of the collencytes and microangium in the dermis layer was typical. On day 30 post-treatment, epithelial tissues showed a remarkable degree of regeneration (Figure 1.2.2.4a), and skin structure was virtually normal (Figure 1.2.2.4b).

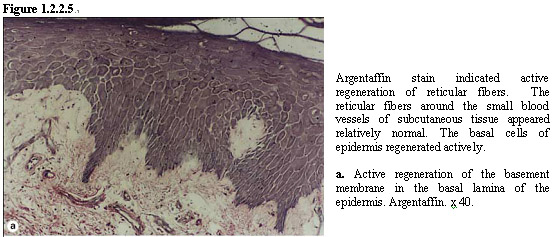
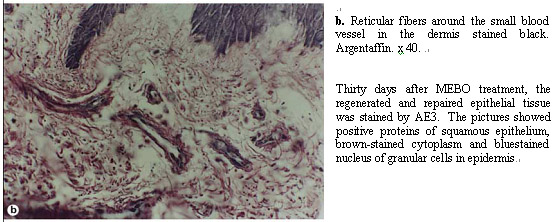
Twenty days post treatment with MEBO, immunohistochemical examination of the wound tissue was performed and the results showed the clear appearance of collagenous fibers in epithelial tissue and subcutaneous tissue (Figure 1.2.2.5).
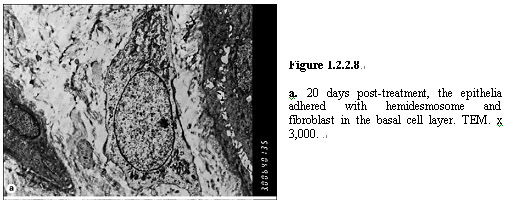
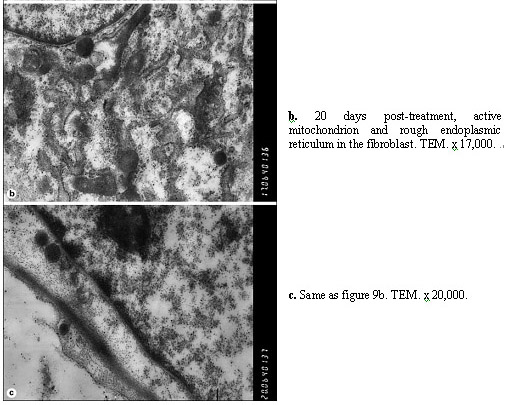
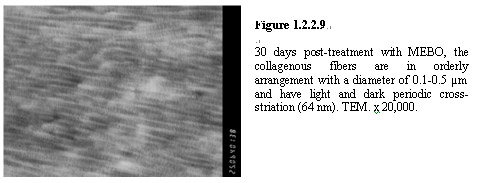
Twenty (20) days post-treatment, appearance of the hemidesmosome junction between the basal cell layer and epithelia was observed. Active mitochondria and RER in fibroblasts also appeared (Figures 1.2.2.8a-c). Thirty (30) days post-treatment with MEBO ointment, with the regeneration and repairing of epithelium almost complete, collagenous fibers were mature with a diameter of 0.1-0.5 µm and arranged in an orderly fashion (Figure 1.2.2.9). Light and dark periodic cross-striation (64 nm) was also observed. No pathomorphological changes of collagenous fibers such as distortion, helicoid (whirlpool) or cauliflower-like form were observed. After wound healing, functional exercises and physiotherapy of the lower extremities were performed. MEBO wound ointment was used continuously as regular skin oil. The patient healed and was discharged home on day 45 postburn.
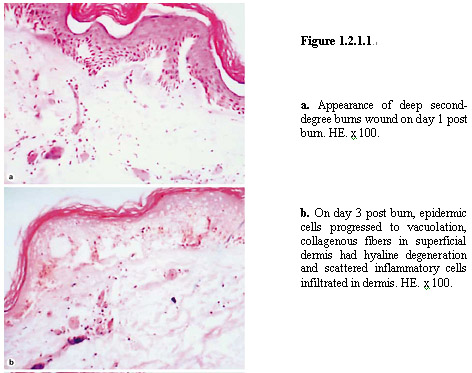
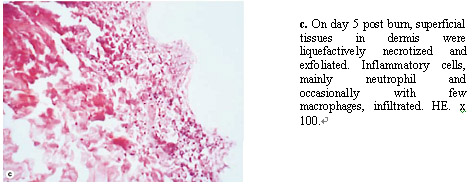
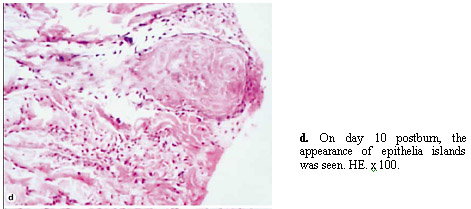
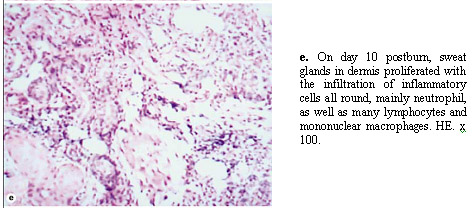
To study the physiological healing process, histological examination was performed on tissue samples taken from deep second-degree burn patients under the treatment using MEBT/MEBO. Xu “Physiological Healing Procedure and Histological Observation on Deep Second-Degree Burns Treated with MEBO” Burns Regenerative Medicine and Therapy, 1st ed., Basel: Karger; 2004. p.106-111.
Six cases were enrolled throughout the study, 5 males and 1 female, aged from 21 to 36 years-old. Total burns surface area varied from 12% to 45%, with an average of 24.33±12.37%. All patients were admitted within 6 h post-burn. After admission, patients received fluid resuscitation and antibacterial therapy on the basis of burn severity. Burns wounds were applied with MEBO at a thickness of 1 mm, which was repeated every 4-6 h till wound was healed.
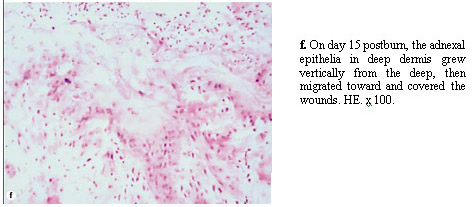
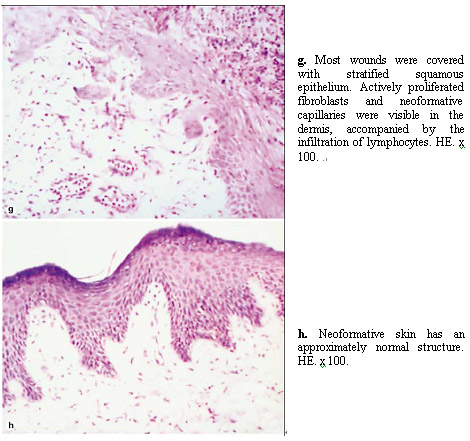
As shown in Figure 1.2.1.1, the tissue at the wound site underwent dramatic patho-morphological changes during the treatment using MEBT/MEBO. Under the conditions provided by MEBO wound ointment, pathological changes of the deep second-degree burn wounds can be divided into three stages: (1) denaturation and necrosis of injured tissue, (2) liquefaction and discharge of the denatured and necrotic tissues, and (3) restoration of physiological structure and function of the skin. These stages may overlap. As shown in Figure 1.2.1h, the newly regenerated skin has virtually an identical morphology and structure to that of non-injured skin. No skin grafting was performed.
During the past twenty years, several controlled clinical trials have been conducted, and thousands of clinical observations and reports have been published on application of MEBT/MEBO to the treatment of wound patients. MEBO has been shown to maintain burn wounds in moist, reduce water evaporation from burn wounds, promote microcirculation in wounds, limit progressive damage after burn, facilitate liquefication and discharge of the necrotic tissues, reduce secondary injuries caused by aggressive surgical excision, prevent wounds from infection, and, furthermore, introduce regeneration of skin tissue over the viable tissue on wounds. The results from extensive controlled clinical studies, along with clinical observations in thousands of burn and chronic wound patients, have demonstrated that MEBO reduces both the physical and psychological pains during treatment, accelerates wound healing process, minimizes scarring, reduces medical costs, and provides better quality of life for wound patients.
During the treatment, MEBO wound ointment is applied to the surface of the wound at 0.5-1 mm in thickness. The wound area is left exposed and the wound bed is kept in moist by the ointment, in contrast to conventional practice that the wound is occluded by dressing or exposed to dry out. This is referred to as Moist Exposed Burn Therapy (MEBT). Every six to twelve hours the wound is cleaned, and liquefied necrotic tissue with MEBO ointment is wiped off followed by reapplication of MEBO ointment. This regimen is repeated until the wound is healed.
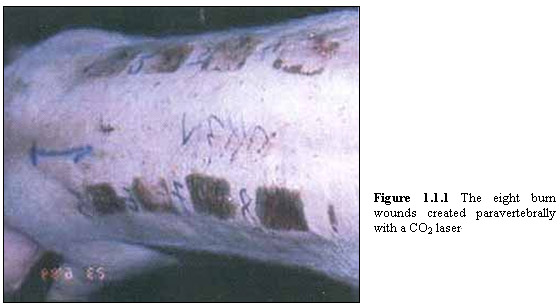
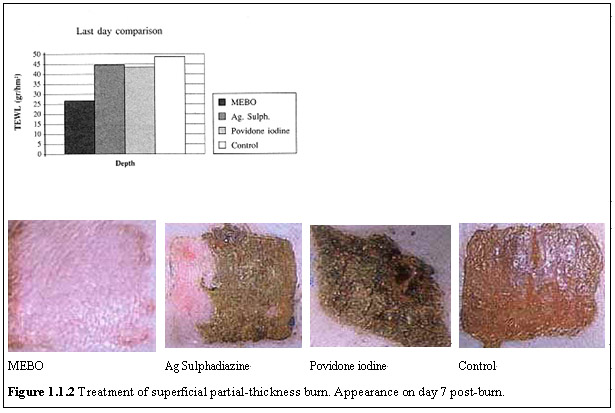
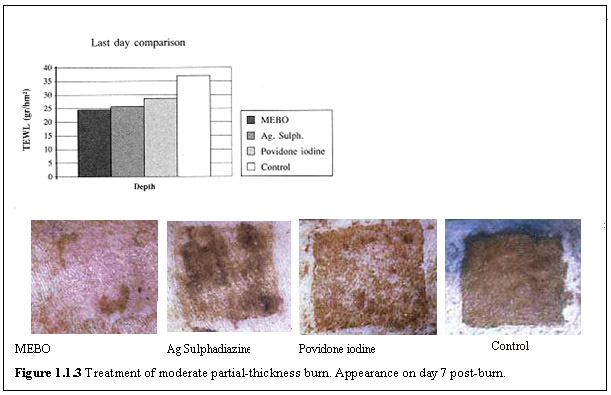
To evaluate the efficacy of MEBO wound ointment on tissue repair and regeneration, preclinical studies were carried out in pig models for burn wounds as compared with that of local wound care agents commonly used in wound treatment. Ioannovich et al. “Moist Exposed Burn Therapy: Evaluation of the Epithelial Repair Process (an Experimental Model)” Annal of Burns and Fire Disasters 2000: XIII (J):3-9. Eighty (80) partial-thickness burn wounds on 10 Ladrace-Pietrenne young pigs were induce by CO2 laser.
As shown in Figure 1.1.1 below 8 partial-thickness burn wounds of different depths measuring 5 x 5 cm were inflicted on either side of the paravertebral region in each pig (total number of burn wounds: 80).

Burn injury is a three-dimensional wound that causes massive tissue loss in the victim. Treatment of burn wounds involves a unique combination of modalities. In addition to topical wound care needs, the patient is at risk for numerous systemic complications associated with the absence of large amounts of epidermis and/or dermis. The goal is not only to save the patient’s life but also to restore the structure and function of the body so as to prevent or minimize disfigurement and disablement.
In comparison, currently for deep partial thickness burns (extending into the reticular layer of the dermis) and full-thickness burns (extending through the dermis and into subcutaneous tissue), unless very small in size, the standard treatment modality is to use skin grafts to close the wounds. Prior to the skin grafting, the wound bed is usually prepared by treating with daily or twice-daily dressing changes with topical antimicrobial application to control the growth of microorganisms and prepare the wound for grafting. Honari (2004) Crit. Care Nurs. Clin. North. Am. 16:1. Bryant & Nix (2007) Acute & Chronic Wounds: Current Management Concepts, Chapter 18 by Jill Evans, 3rd Ed., Mosby, Inc.
Successful skin grafting could repair the wound through revascularization with sprouting and budding of vessels in both donor and recipient sites. Falabella & Kirsner (2005) Wound Healing, Chapter 41 “Skin Grafting: Surgical Techniques” by Yamaguchi et al., Taylor & Francis Group, Boca Raton, FL. However, in the grafted epidermis and dermis, the function of the appendages of the skin such as hair follicles, nerves, sweat glands, and sebaceous glands is severely compromised, if not completely lost. Thus, although the patient’s life is saved and wound closed, a significant loss of physiological functions of the skin results and, for patients with large area burns, decrease in morbidity is inevitable.
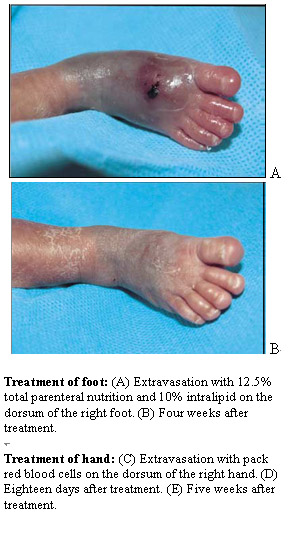
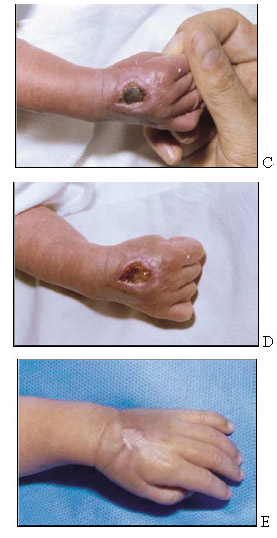
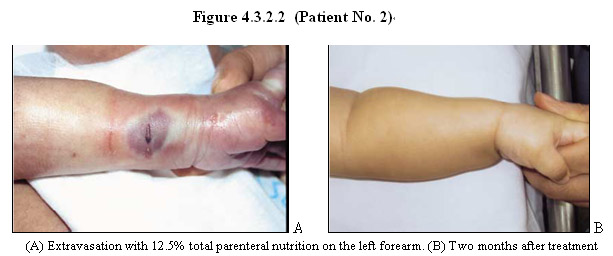
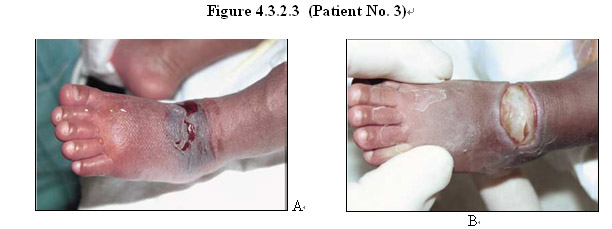
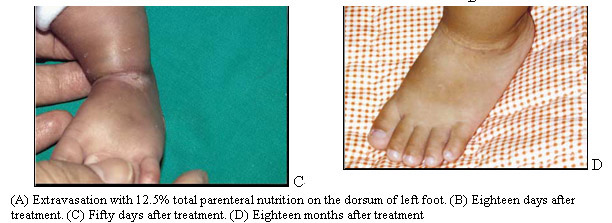
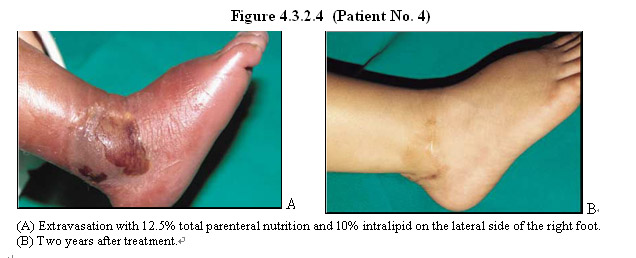
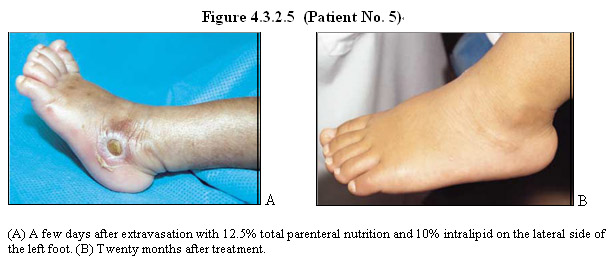
MEBO wound ointment has also been used successfully to treat extravasation injury during parenteral hyperalimentation of infants, especially preterm infants. As described by Cho et al. (2007) “Successful combined treatment with total parenteral nutrition fluid extravasation injuries in preterm infants” J Korean Med Sci 22: 588-94, five (5) premature infants with wounds of hyperalimentation fluid extravasation were treated with MEBO wound ointment in combination with an antibacterial ointment (Terramycin ophthalmic ointment). Table 4.3.1 summarizes the results of the treatment.
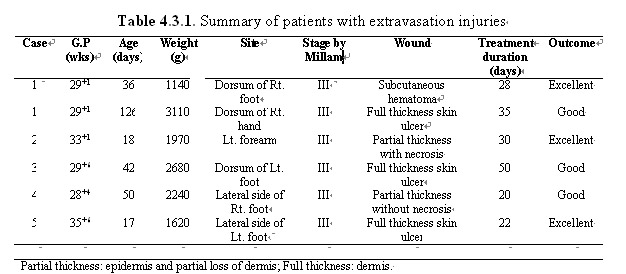
As shown in Figures 4.3.2.1-5, wounds of these 5 patients had healed completely within about 1 month with a small size of contracture without functional abnormality. At 2 years follow-up, the wounds had healed completely without any sequel.
Figure 4.3.2.1 (Patient No. 1)
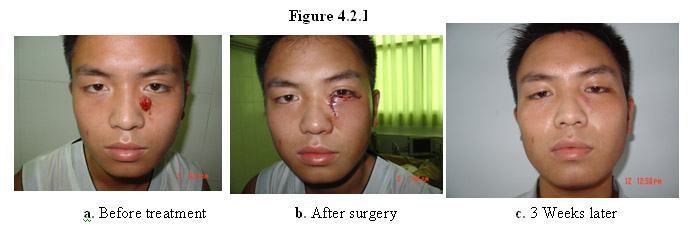
As shown in Figure 4.2.1, a wart on the face of this patient was surgically removed. The sutured wound was treated with MEBO wound ointment. Three weeks later the scar on his face was barely visible.
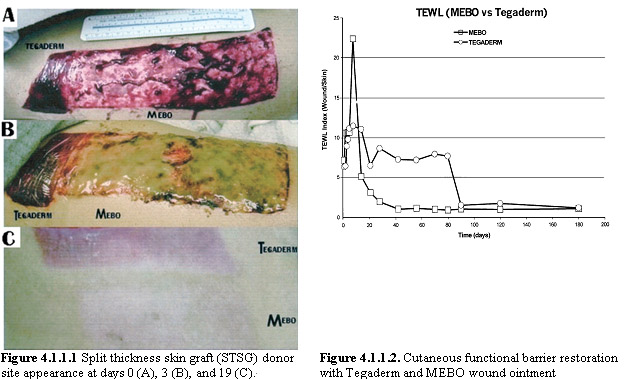
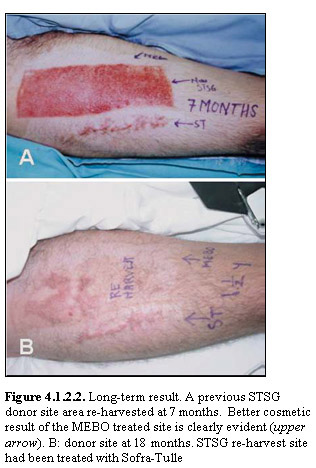
Clinical studies of the effects of MEBO wound ointment on the wounds of skin graft donor sites have been carried out to evaluate scar quality and physiologic barrier function restoration, as compared with Tegaderm, a semipermeable membrane occlusive dressing and with Sofra-Tulle, an antibiotic impregnated Vaseline gauze. Atiyeh et al. “”Scar quality and physiological barrier function restoration after moist and moist-exposed dressings of partial-thickness wounds” Dermatol Surg 2003 Jan; 29(1):14-20. Atiyeh BS, et al. “The effect of moist and moist-exposed dressings on healing and barrier function restoration of partial-thickness wounds” “ European Journal of Plastic Surgery 2003; 26(2): 5-11.
As shown in Figure 4.1.1.1, compared with Tegaderm application of MEBO wound ointment to split thickness skin graft (STSG) donor sites resulted in earlier anatomic healing with significantly superior cosmetic appearance of the resultant scars over 6 months of follow-up. Further, average functional barrier recovery time was 67.4±13.368 days for MEBO and 150±46.476 days for Tegaderm (Figure 4.1.1.2).

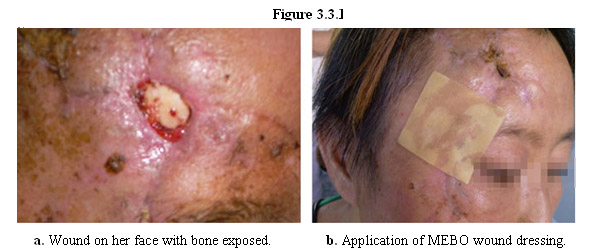
In this case, MEBO’s regeneration therapy and wound dressing was used to treat a earthquake victim with wound on her face and bone exposed (Figure 3.3.1). By applying MEBO wound dressing to her wound, the skin and underlying tissue were regenerated without leaving apparent scars on her face.

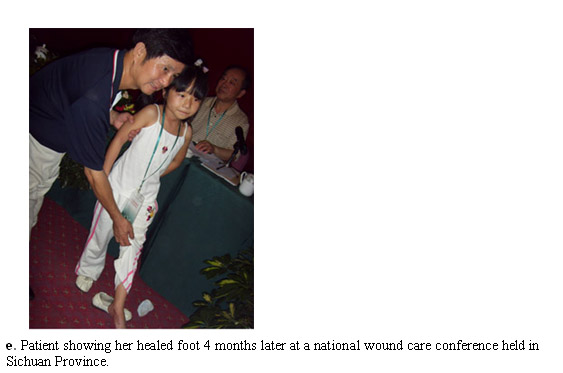
The left foot of a nine year-old girl was severely injured during the May 12 earthquake with an open, infected wound (Figure 3.2.1). Dr. Xu supervised her treatment by using MEBO’s regeneration therapy coupled with negative pressure wound therapy provided by an Israeli medical rescue team volunteering in the quake zones. Under the condition provided by MEBO ointment, a skin flap was successfully engrafted to allow regenerative healing of her wound, thereby avoiding amputation of her leg.


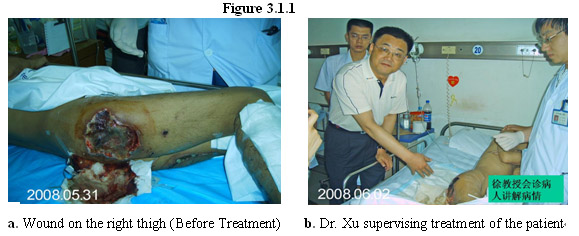
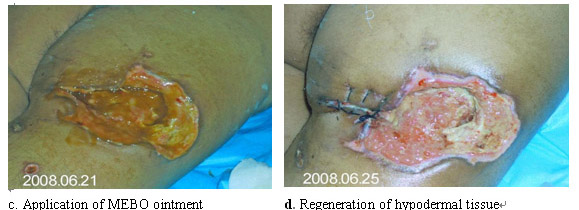
On May 12, 2008 strong earthquakes of 7.9 magnitude struck Sichuan Province of China, which caused ninety thousands of death and wounded about a quarter million people. Dr. Xu led China’s wound experts to the disaster zones and personally supervised treatment of many wounded victims by using MEBO’s regeneration therapy in conjunction with MEBO wound ointment and dressing.
Shown in Figure 3.1.1 is a quake victim (age 36) with multiple open, deep wounds, especially in the right thigh that sustained a 25x20 cm2 wound injury with muscular necrosis and severe sciatic nerve damage. Three months later regeneration of hypodermal tissue under the condition provided by MEBO ointment resulted in significant restoration of structure and function of his leg, including sciatic nerves.

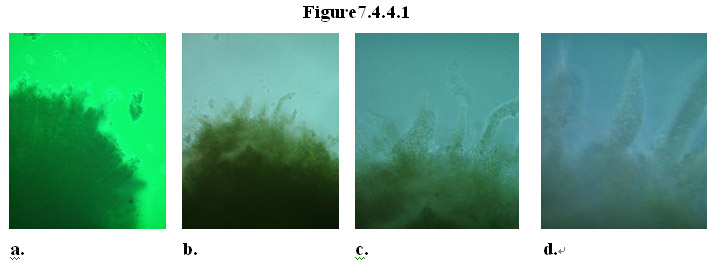
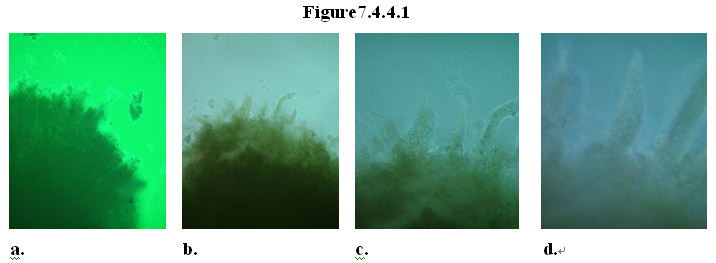
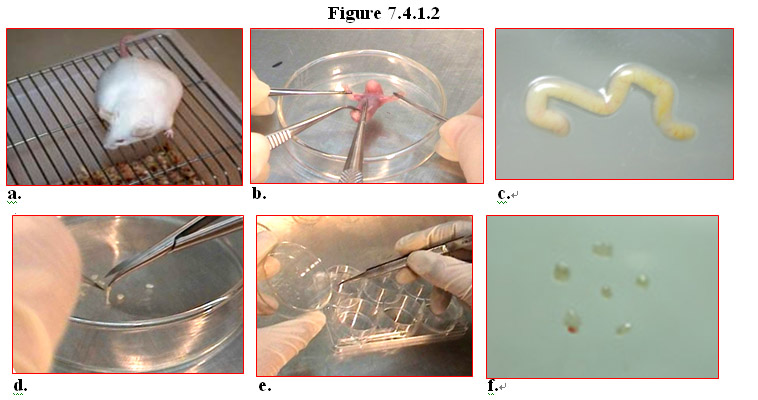
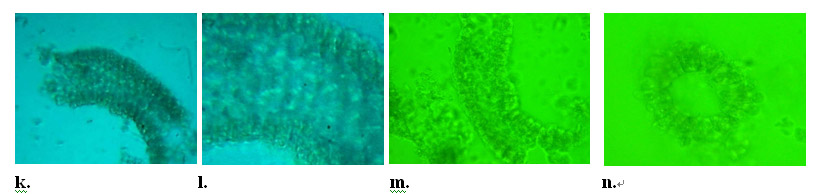
To further test the ability of the MEBO regenerative nutrients to facilitate cloning of physiologically correct tissue in vitro, experiments were conducted on explants of mouse intestine. Explants of mouse intestine were obtained and a few villi on the explants were excised and cultured in normal cell culture medium. The cultured explants were divided into two groups: test group and control group. The MEBO regenerative nutrients were added to the cultures in the test group, while the control group did not receive any supplement.
As shown in the panels in Figure7.4.4.1a-d, in the treatment group the explants not only survived but also grew new villi from the wound where the original villi had been removed. By day 6, nascent structure of villus started to appear on the wound, and by day 8 regeneration of multiple new villi with the same physiological structure as the original ones was complete. By contrast, explants in the control group gradually disintegrated and died in the culture (Figure7.4.4.2a-d).
So far our extensive literature search has not found reports of such results of regeneration of villus from explants cultured in vitro. These results are significant as they once again demonstrate that the MEBO regenerative nutrients are able to promote regeneration of injured tissue and organ, consistent with the clinical results obtained from wound and ulcer patients. Scientifically groundbreaking is the fact that under the condition provided by the MEBO regenerative nutrients, normal somatic cells can behave like stem cells to proliferate vigorously and differentiate orderly to produce multiple cell types which eventually form tissue with physiologically correct structure, both in vivo and in vitro.
These findings are illuminating in that the MEBO regenerative nutrients can be delivered not only topically but also systemically to facilitate regeneration of injured or aged tissue and organ in the body.
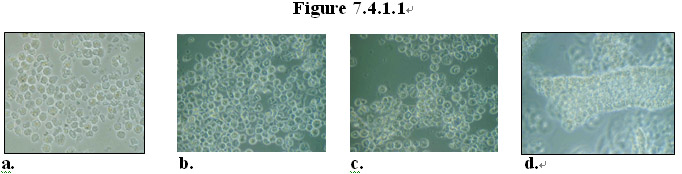
Normal human living intestine was obtained from surgical operations, and enzymatically digested so as to obtain dispersed single cells from the intestine samples. The suspended intestinal cells were cultured in MEM medium and divided into two groups: test group and control group. The MEBO regenerative nutrients were added to the cultures in the test group, while the control group did not receive any supplement. Every 3 days the old growth medium was discarded and fresh growth medium same as the first round was added to the cultures in the respective groups.
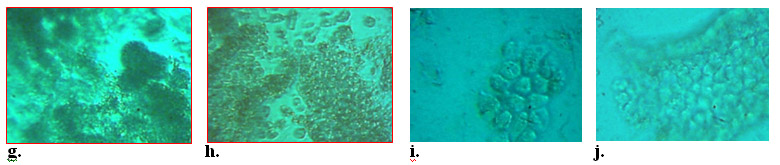
After 55 days of culture, in the treatment group the cells had grown into groups of cells appearing in various forms, including proliferation and differentiation of the cells isolated from human intestine samples. As shown in Figure 7.4.1.1a-c, in some areas, some of cells formed clusters that appeared to look like pieces of tissue. Surprisingly, it was observed that in some areas, tissue pieces resembling a fully assembled villus structure appeared in the culture Figure 7.4.1.1d. In comparison, most cells in the control group had died by Day 55.
These results are groundbreaking as they demonstrate that the MEBO regenerative nutrients can sustain vigorous proliferation and facilitate orderly differentiation of somatic cells for a long period of time to form multiple cell types that are linked together to form tissue with physiologically correct structure in the culture. From single, isolated cells from human and mouse intestines at least 4 types of cells are formed: entercytes, mucus-secreting goblet cells, enteroendocrine cells, and Paneth cells which are originated from epithelial stem cells in the crypts of the intestine. Although it remains to be ascertained the nature of the single, isolated cells that produced the multiple cells types in the culture containing the MEBO nutrients, it is significant that physiologically correct tissue has been cloned in vitro from single cells isolated from intestines. To our best knowledge, there is no report from others with the same results.
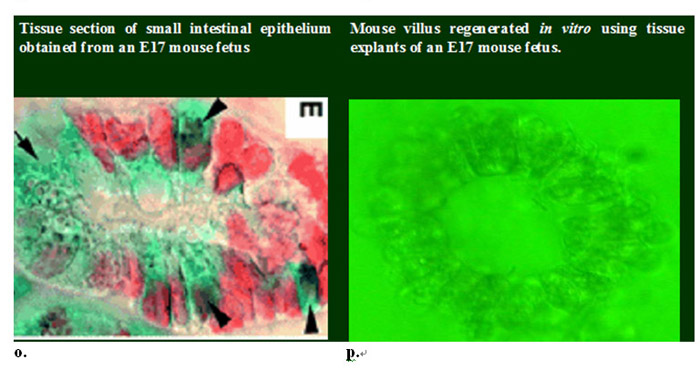
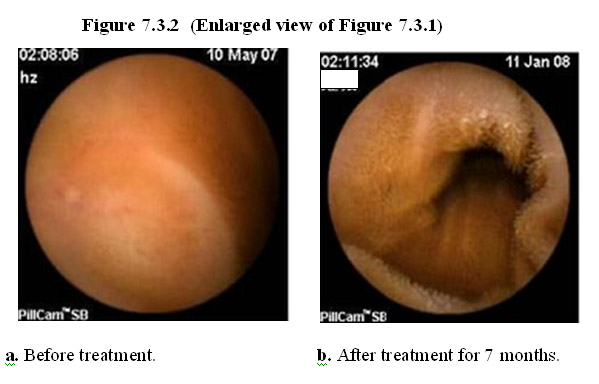
As shown below in Figures 7.3.1 and 7.3.2, healthy adult humans, even if having degenerated/atrophic shortened villi on the GI lining due to aging, can still benefit from the regenerative power of the MEBO nutrients which promote re-growth of lush, longer villi (which are associated with a more youthful human body). By using the MEBO nutrients to regenerate the GI lining without scar formation, the GI system is revitalized functionally to allow better absorption of nutrients to the body, which, in turn, leads to nourishment of the body systematically.
Case 1: Female, age 55, healthy.
Built upon MEBO’s innovative technologies and products for the regeneration of wounded skin that leads to restoration of normal skin structure and function, MEBO has developed a series of products that are formulated for oral delivery and can be taken conveniently in the form of soft gel capsules by users to maintain the integrity of or to repair/regenerate the mucosal tissue without scar formation. Similar to the process of regeneration of the epithelium of the skin, repair or regeneration of damaged or eroded epithelium on the mucosal lining can be achieved by activating and sustaining intrinsic regenerative potential of the body and cultivating stem cells of the body in situ, i.e., right at the site of ulcerative lesion.
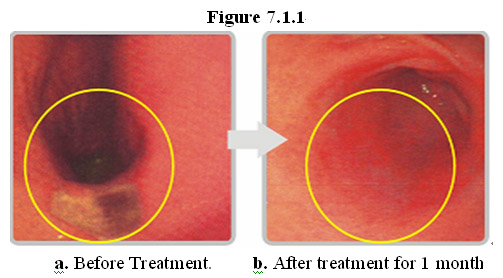
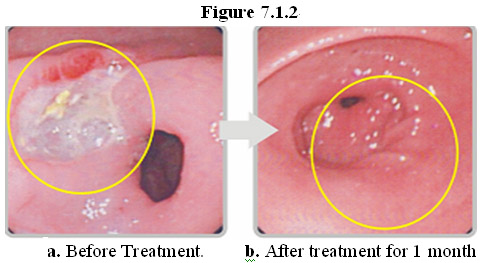
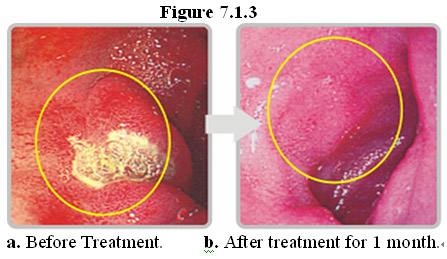
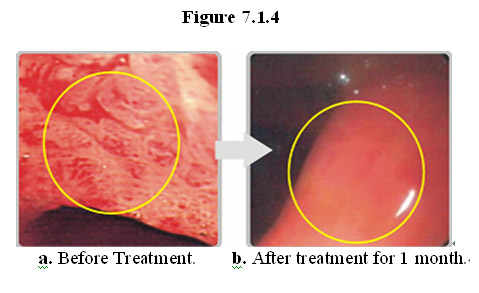
As shown below, the mucosal tissues of those who suffered from various GI disorders (such as gastric ulcer, duodenal ulcer and erosive gastritis due to the side effects of chemotherapy and radiation) can be regenerated after a month of taking the MEBO regenerative nutrients. The newly regenerated mucosa is scarless.
Case II: Female, age 50, peptic ulcer in the antrum of the stomach.
Case III: Male, age 41, duodenal ulcer.

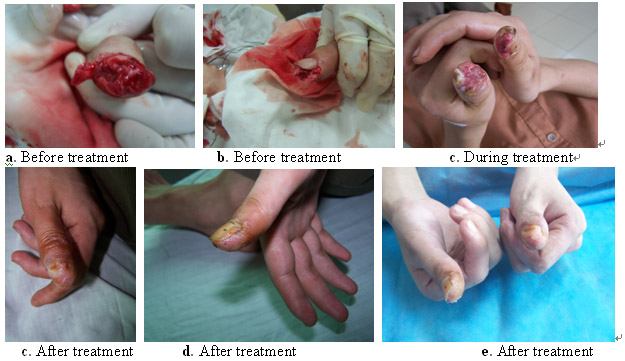
Case 1: Male, age 36, left middle and ring fingers crushed by concrete plane.



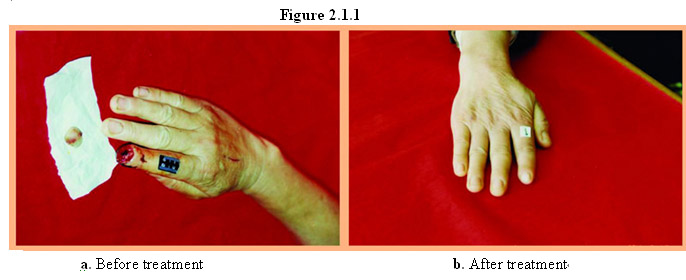
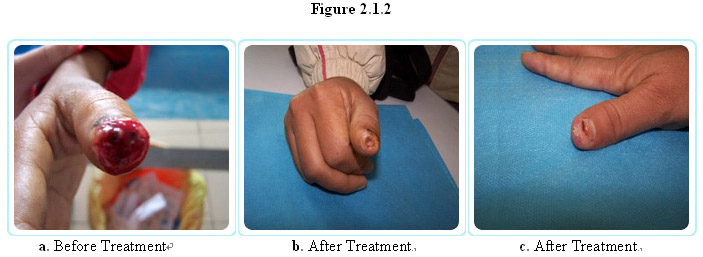
Case 1: Female, age 57, right index fingertip bitten off (Figure 2.1.1a), in-patient treatment with MEBO wound ointment for 15 days at a clinic, followed by out-patient treatment using the ointment. Half a year later her injured finger was completely regenerated with restoration of sensory functions and shape and form (Figure 2.1.1b). The fingerprint of the new finger tip was certified by the local authority (Figure 2.1.1c) as being identical to the finger print prior to the injury.


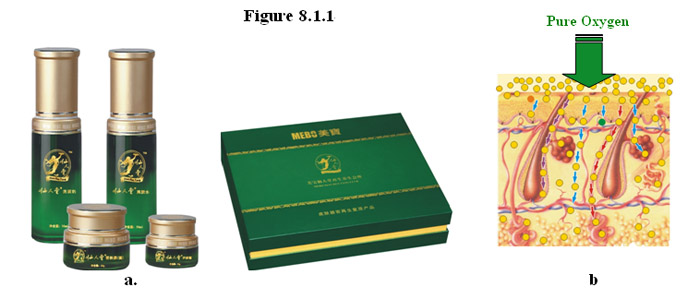
Having achieved remarkable clinical success of regeneration of the skin and underlying tissues, MEBO has further developed a series of products (Figure 8.1.1a) and technologies for restoring normal structure and function to the skin that has been compromised due to aging. The products are topical agents containing the MEBO regenerative nutrients in isotonic formulations for ready absorption by the skin. To accelerate the regeneration and maximize delivery of the nutrients to the skin and underlying tissues, the products were delivered directly to the skin by using moderately pressured oxygen (Figure 8.1.1b). Such non-invasive procedure is conducted in a setting of medical spa inside MEBO’s Beijing headquarters over the course of 3 months.
The results from our studies are surprisingly encouraging. As shown in Figure 8.1.2 below, the skin of aged adult humans (age >50) can not only be renewed but also be restoratedd, i.e., reversed to a more youthful state.
This is a 55 year-old woman having the skin typical for this age group (Figure 8.1.2a):
i) The epidermis: Rough, uneven surface, lack of luster, obvious thinning of the cornified layer and epidermis, disorderly surface pattern, poor blood circulation, limpy facial hair and lack of skin vitality;
ii) The dermis and underlying tissue: loose, collapsed tissue, manifest more squared facial structure due to lack of support of the skin, and lack of suppleness and vitality.
After the 3 months of topical treatment with the MEBO regenerative nutrients, her skin has been changed significantly in the following aspects (Figure 8.1.2b):
i) The epidermis: smooth, radiant surface, full of luster, obvious thickening of the epidermis, orderly and clear surface pattern, good blood circulation, erect facial hair, and full of vitality;
ii) The dermis and underlying tissue: supple, full dermis and underlying tissue tightening and supporting the facial structure to adopt a fuller, oval shape, radiant complexion.

These results indicate that her skin has been restorated to have the structure and function of the skin of a person at least 20 years younger.
In the same woman, significant results were also obtained in the restoration of the skin and underlying tissue of her neck. As shown Figure 8.1.3a below, before the treatment, the skin of her neck manifested the signs of aging, more typical of the skin of a person in the 60’s or 70’s: rough, bumpy, lusterless surface, severely loose, thinning dermis, showing of deep layer blood vessels, and lack of vitality.
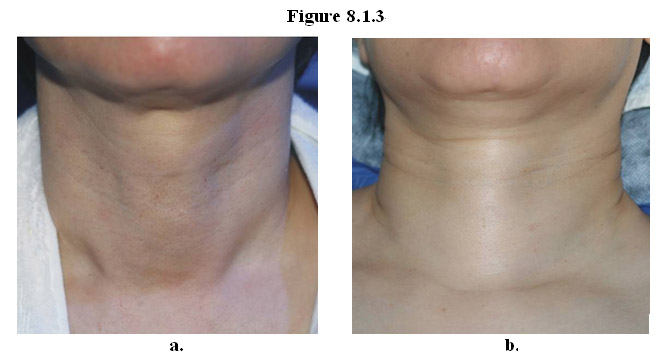
After 3 months of treatment (Figure 8.1.3b), consistent with the results of her face, the skin and underlying tissue of her neck have been completed changed: smooth, radiant surface, thickening of the epidermis, supple, fuller dermis, shallow necklines, tightening of the skin, and no showing of deep layer blood vessels, and full of vitality.
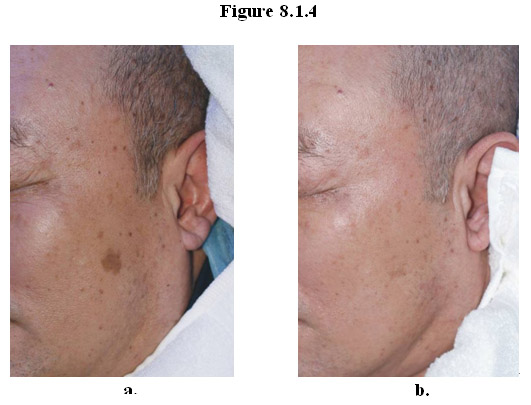
The same technique has been used to restore the skin of an elderly man. As shown Figure 8.1.4a below, before the treatment his skin showed typical signs of aging: hyper-pigmentation, numerous dark age spots, loose skin, and lack of vitality. After 3 months of treatment (Figure 8.1.4b), the condition of his skin was significantly changed with substantial elimination of age spots, reduction in hyperpigmentation, improved complexion and vitality.
Looking beyond the skin surface, in the dermis of young skin collagen fibers form tight, orderly (Figure 8.1.4b) bundles whereas in collagen fibril bundles in the aged skin are much looser and more disorganized (Figure 8.1.4a).
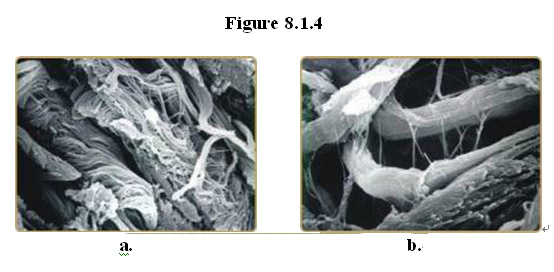
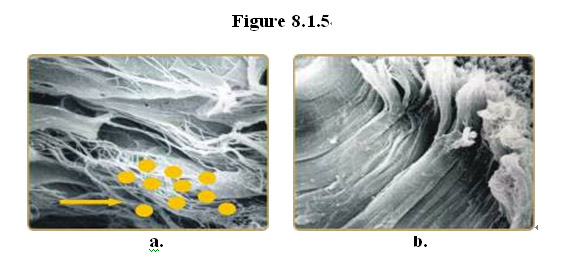
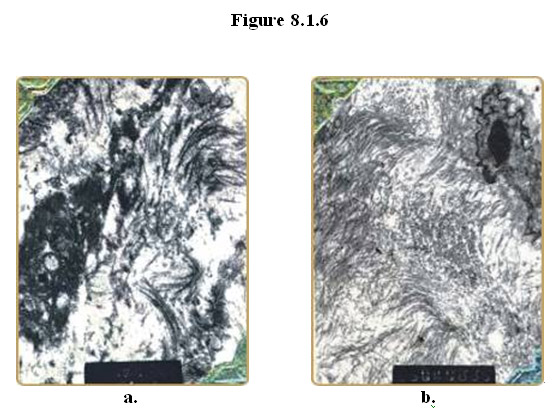
Examination of the skin sample under a scanning electron microscope revealed that delivery of the MEBO regenerative nutrients directly to the aged skin and underlying tissue results in regeneration of fibrocytes and restoration of normal, more youthful architecture of collagen fibrils. As shown in Figures 8.1.5a and 8.1.6a, typical aged skin has loose collagen fibrils arranged in a disorderly and chaotic configuration and shows signs of collagen dissolution and cytolysis of fibrocytes. After topically delivery of the MEBO regenerative nutrients to the skin, uniformly thick collagen fibers arranged orderly in dense, tight bundles parallel to the skin surface (Figures 8.1.5b and 8.1.6b).
Formally commenced on Janurary 25, 2008 in China, MEBO initiated a large-scale clinical studies of end-stage cancer patients who had failed all medical interventions and given up upon further medical treatment (as certified by patients’ oncologists). About 300 end-stage cancer patients, exhibiting a variety of different cancer types (including lung, liver, gastrointestinal (esophagus, stomach, colon, rectal cancer), pancreas, breast, prostate, uterus/cervix, ovarian, thymus, neuroblastoma) were enrolled and provided with MEBO regenerative nutrients. Preliminary results are extremely encouraging: most patients (~80% overall 1-year survival rate) not only survived but also improved significantly in all detectable indexes including the body weight, reduction in tumor size, elimination of leukemia cells (in patients with relapsed leukemia), and improvement in mobility and vitality.
For example, a 58 year-old female patient was diagnosed with right lung cancer that had metastasized to the bone, and was treated with chemotherapy for 3 courses without surgical operation. The treatment modality did not improve her condition and she still coughed up blood (haemoptysis) and had a persistent pain in her right ribs. She subsequently gave up upon such treatment and started taking the MEBO regenerative nutrients in February 2008. Four months after her overall condition improved: haemoptysis disappeared; rib pains alleviated; and appetite, complexion and vitality improved (Figure 10.10.1a). The tumor in her right lung regressed from a size of 30x43 mm to 27x29 mm.
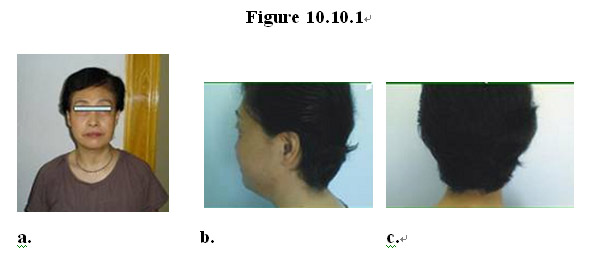
Remarkably and surprisingly, after 4 months on the MEBO regenerative nutrients the patient who had suffered from hair loss due to chemotherapy started grow thick, lush and lustrous black hair (Figure 10.10.1b-c) that appeared to be even healthier than a typical woman of her age. The texture of her skin also improved, becoming suppler and smoother. Interestingly, her breasts seemed to become firmer and vaginal discharge that had disappeared 7-8 years ago reappeared.
Currently these patients have voluntarily elected to continue getting nutritional support from MEBO and their monthly reports are gathered by MEBO for further analysis.
The results obtained from MEBO’s 1-year clinical studies, although preliminary, are very encouraging. They demonstrate that by using the MEBO regenerative nutrients as nutritional support, cancer patients, even if at a late or end stage, can still benefit from this unique modality in the absence of conventional medical intervention or after failure of all medical interventions. The patients not only survived but also enjoy better quality of life. In some cases, such as relapsed acute leukemia and gastrointestinal cancer, the patients have had complete remission and remarkably improved vital indexes. Continuous taking of the MEBO nutrients also seemed to have certain rejuvenating effects on the patients who manifested certain degree of tissue/organ regeneration during the course, such as growing healthier-, younger-looking skin and hair.
These preliminary results obtained by MEBO in its cellular, tissue and human studies should shed new light on cancer research, prevention and treatment. Since the 1950’s, despite the enormous amounts of funding targeted for cancer research by the governments and private entities throughout the world, it is yet far away from claiming victory in the ongoing war against cancer. It has been predicted that one in two men and one in three women are likely to die of cancer. World Fact Book, Central Intelligence Agency, Office of Public Affairs, Washington, D.C., July 2006. Thus, it can be estimated that, if anti-cancer agents with long-term curative effects are not found soon, particularly for advanced metastatic cancers, about 2.7 billion people would die of cancer, considering there are about 6.5 billion people in the world today. In the United States, and in the rest of the world, people are still looking for the first “Magic Bullet” that will consistently destroy in different patients both primary and metastatic cancers regardless of their tissue of origin while exhibiting minimal toxicity to the human host. Pederson (2007), supra.
Against this grim background, MEBO beckons as a bright beacon for the world. Built upon solid scientific and clinical foundations and with superior safety profiles, the MEBO approach of utilizing its dual-functional regenerative nutrients and technologies offers enormous hope for humanity as a whole, and globally it will have a profound impact on the currently overburdened health care systems and overstressed economies in both developed and developing countries.
Oral formulations of the MEBO regenerative nutrients have also been used to restore structure and function of tissues and organs of cancer patients that are damaged by the side effects of chemotherapy and radiation therapy.
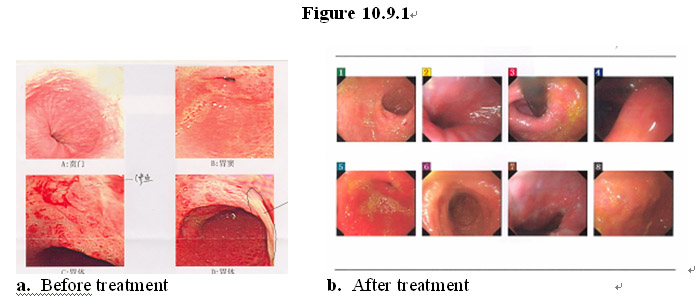
As shown in the gastrointestinal endoscopic images in Figure 10.9.1a, a patient (male, age 59) had pancreatic cancer that had metastasized to the stomach and sustained extensive damage of the gastric lining due to chemotherapy and radiation, leading to the development of erosive gastric ulcers. After taking the MEBO regenerative nutrients, his gastrointestinal wall and other GI lining have been regenerated with normal, healthy mucosa and underlying tissues (Figure 10.9.1b).
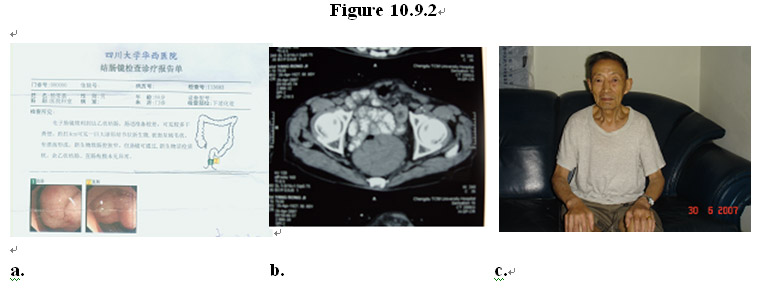
In another example, as shown in the gastrointestinal endoscopic images in Figure 10.9.2a-b, a patient (male, age 80) was diagnosed with rectal cancer with the tumor mass located at 4 cm above the anus, causing ulcer lesion there. After taking the MEBO regenerative nutrients for 3 months the tumor disappeared and the rectum is regenerated with normal, healthy mucosa and underlying tissues (Figure 10.9.2c).
Oral formulations of the MEBO regenerative nutrients have been used as nutritional support for end-stage cancer patients who have given up medical treatment of cancer.
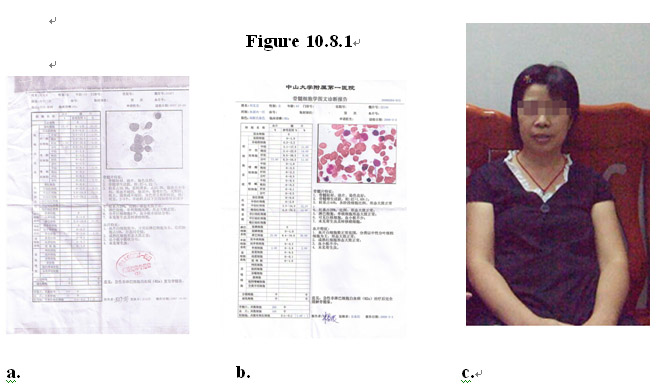
As shown in Figure 10.8.1, a patient (female, age 43) was diagnosed with acute myeloid leukemia (AML-M2a) 6 years ago and went into remission after treatment with chemotherapy. In October 2007 her leukemia reoccurred and was resistance to treatment with chemotherapy. As shown in Figure 10.8.1a, peripheral blood and bone marrow smear tests showed that cells in the granulocyte series accounted for 35.5% with the myeloblast count in her bone marrow increased to 25.5% with varied sizes and irregular morphology.
Starting January 2008 she gave up medical cancer treatment and started taking the MEBO regenerative nutrients as nutritional support. One and a half months later, peripheral blood and bone marrow smear tests showed that cells in the granulocyte series accounted for 44% with no myeloblast detected, and cells in all phases showed generally normal ratios and morphology; red blood cell series accounted for 26%; and cells in all phases showed generally normal ratios and morphology (Figure 10.8.1b). After 3 months on the MEBO regenerative nutrients, her overall condition improved significantly with healthier complexion, better quality sleep, and gained about 5 Kg of weight (Figure 10.8.1c).
These results demonstrate that systemic uptake of the MEBO regenerative nutrients can cause complete remission of relapsed AML and full restoration of normal hematological cell counts, ratios and morphology. Such results are extremely encouraging and shed new light into innovative treatment of late-stage leukemia without intervention using chemotherapy or hematological/stem cell transplantation. The fact that the patient’s hematological cell counts, ratios and morphology have been fully restored suggests that the MEBO regenerative nutrients may act on the source of all hematological cells: the hematopoietic stem cells, by promoting proliferation and differentiation of the stem cells that follow the correct, normal lineages while inducing death of leukemia cells, thereby regenerating the hematological system and eradicating cancer. Further human studies led by MEBO are under way in larger patient populations in China.
Topical formulations of the MEBO regenerative nutrients were used to successfully treat various forms of skin cancer, including basal cell carcinoma and squamous cell carcinoma.
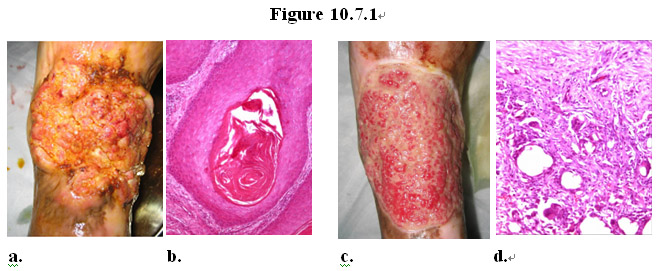
As shown in Figure 10.7.1, a patient with squamous cell carcinoma (Figure 10.7.1a) on his leg was treated with a topical formulation of the MEBO regenerative nutrients. Twenty (20) days later pathological examination of the tissue at the cancer site revealed that the original cancerous tissue (Figure 10.7.1b) disappeared, replaced with normal healthy granulation tissue (Figure 10.7.1 c-d).
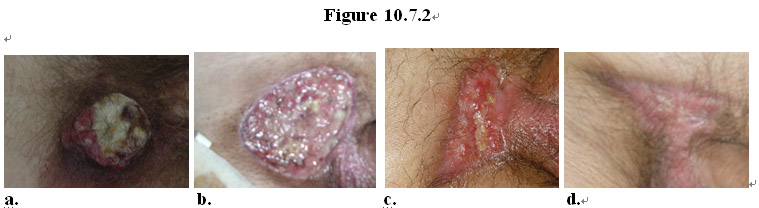
As shown in Figure 10.7.2, a patient with low differentiated squamous cell carcinoma (Figure 10.7.2a) near his genital was treated with a topical formulation of the MEBO regenerative nutrients. Ten (10) days later pathological examination of the tissue at the cancer site revealed that the original cancerous tissue disappeared, replaced with normal healthy granulation tissue (Figure 10.7.1b-c). Continued treatment with the MEBO product resulted in eradication of the cancerous tissue and healing of the wound (Figure 10.7.1d).
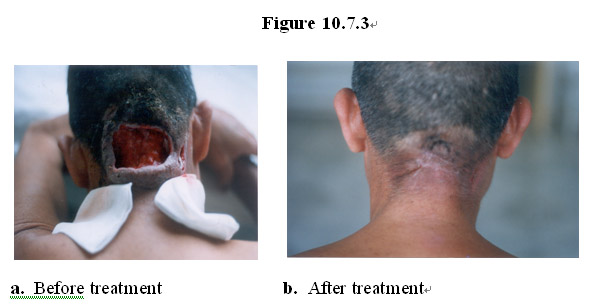
As shown in Figure 10.7.3, a patient with severe erosive, necrotic wound caused by basal cell carcinoma (Figure 10.7.3a) on his neck was successfully treated with a topical formulation of the MEBO regenerative nutrients, resulting in complete eradication of cancerous tissue and healing of the gapping open wound (Figure 10.7.3b).
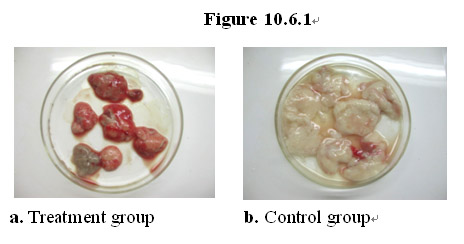
To test the effects of the MEBO regenerative nutrients on the growth of cancer cells in vivo, a standard animal model for highly aggressive malignant cancer growth, mice bearing S180 ascites tumors, was used. When injected into the peritoneal cavity, S180 cells grow exponentially with a generation time of 12-18 hours. Growing primarily in suspension in the peritoneal cavity, S180 cells gradually plug peritoneal lymphatic drainage, leading to accumulation of ascites fluid within 2 weeks. S180 cells can also metastasize into major organs near the peritoneal cavity, such as the liver, kidney, pancreas, lung, stomach, and intestine. Mice that develop ascites normally die in 3-4 weeks. S180-induced ascites represents one of the most aggressive transplantable cancers in experimental mouse models.
In the study, fourteen (14) mice were injected intraperitoneally with S180 cells to induce formation of ascites tumors and 15 days later divided equally into treatment and control group. In the treatment group, seven (7) rats were fed with a regular diet supplemented with the MEBO regenerative nutrients while the control group with just the regular diet. Seventeen (17) days later the mice from both groups were sacrificed and ascites tumors were removed from the peritoneal cavity and weighed.
As shown in Figure 10.6.1a, the average weight from the tumors from the treatment group is about 1 g. In contrast, the average weight from the tumors from the control group is about 3 g (Figure 10.6.1b). These results demonstrate that the MEBO regenerative nutrients are active in the suppression of aggressive tumor growth in vivo.
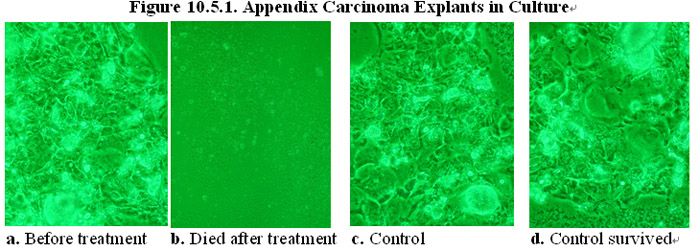
To test the effects of the MEBO regenerative nutrients on cancer cells in solid tumors, in vitro experiments were conducted in a culture containing explants from human solid tumor tissues.
As shown in Figures 10.5.1a and c, explants of human appendix carcinoma tissues were divided into treatment and control group and cultured in normal cell culture medium. In the presence of the MEBO regenerative nutrients, the cancer cells in the treatment group died and the tumor tissue explants disintegrated in the culture (Figure 10.5.1b). In comparison, in the absence of the MEBO regenerative nutrients, the cancer cells in the control group did not die and the explants survived in the culture (Figure 10.5.1d).
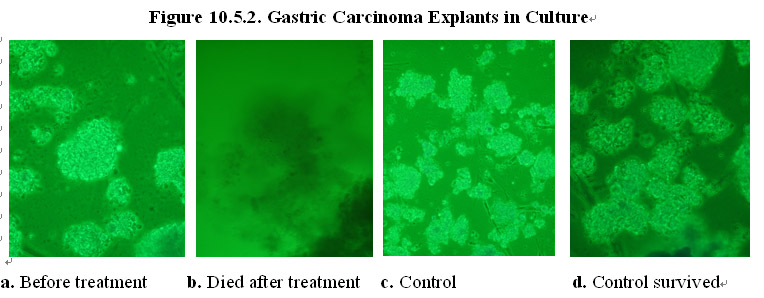
In another experiment, explants of human gastric carcinoma tissues were divided into treatment and control group and cultured in normal cell culture medium (Figures 10.5.2a and c). In the presence of the MEBO regenerative nutrients, the cancer cells in the treatment group died and the tumor tissue explants disintegrated in the culture (Figure 10.5.2b). In comparison, in the absence of the MEBO regenerative nutrients, the cancer cells in the control group did not die and the explants survived in the culture (Figure 10.5.2d).
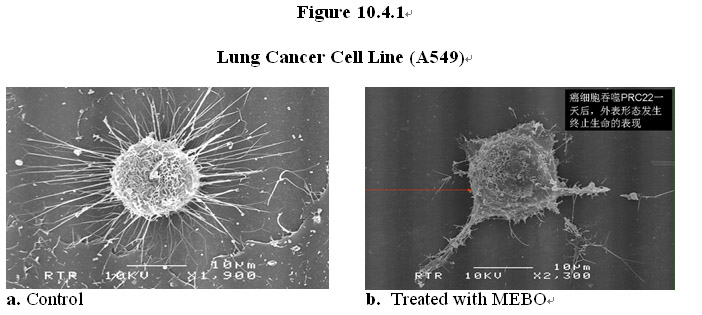
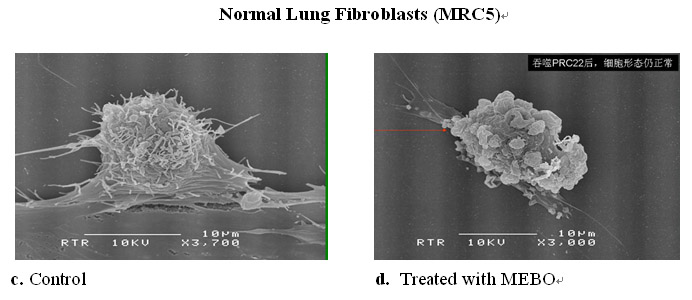
To explore the mechanism of dual functions of the MEBO regenerative nutrients, examination of the cancer cells and normal cells under ultra-fine electron microscope was carried out. A549 lung cancer cells and MRC5 normal lung fibroblasts were cultured in the presence of the MEBO regenerative nutrients for 48 hours and then fixed for microscopic examination.
As shown in Figure 10.4.1 below, under a scanning electron microscope there is a dramatic difference in the cell surface morphology of the cancer before and after exposure to the MEBO regenerative nutrients. The rich microvilli extending from the surface of the cancer cell and attached to the culture plate (Figure 10.4.1a) virtually disappeared and detached (Figure 10.4.1b). In comparison, cell surface morphology in the normal cell appeared to be normal after the treatment with the MEBO regenerative nutrients (Figures 10.4.1c-d).
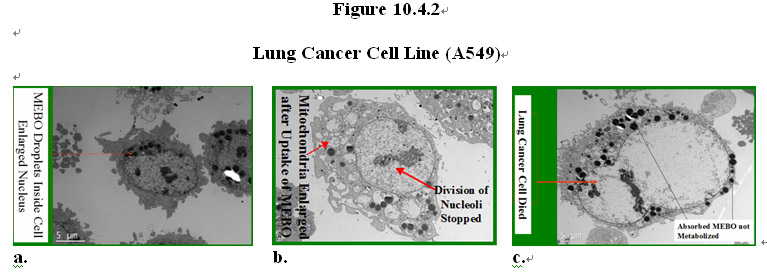
The intracellular components of the cancer and normal cells were examined under a transmission electron microscopy. Dramatic differences were also observed in the response of the cancer and normal cells to the MEBO regenerative nutrients. As shown in Figure 10.4.2, both types of cells readily absorbed the MEBO nutrients that are lipophilic, as shown by the dark dots of oil droplets inside the cells (Figure 10.4.2a). Surprisingly, in the cancer cell, upon uptake of the nutrients into the cytoplasm, it can be observed that mitochondria of the cancer cell were enlarged and swollen while the nucleus stopped dividing (Figure 10.4.2b). The nutrient droplets stayed in the cytoplasm and did not get metabolized before the growth arrest which was then followed by cell death (Figure 10.4.2c).
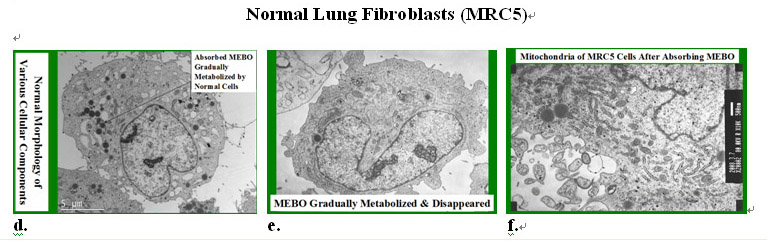
In contrast, in the normal cell the MEBO nutrient droplets were taken into the cytoplasm and gradually metabolized by the cell (Figures 10.4.2d-e). The normal cells not only did not die but also underwent vigorous proliferation as shown by active cell division and increase of cell numbers in the culture. Mitochondria of the normal cell appeared to be normal after uptake of the MEBO regenerative nutrients.
These results demonstrate distinctly differential metabolism of the MEBO regenerative nutrients in cancer and normal cells. The cancer cells absorb the nutrients, which causes enlargement and swelling of mitochondria, the power plants of a cell. As observed under the microscope, the cancer cells subsequently undergo growth arrest which is followed by cell death. It is conceivable that the substantial modification of the structure of mitochondria leads to disruption of their function, leading to a shutdown of the cellular activity and release of pro-apoptotic factors, causing cell death. Importantly, the growth of the normal cells is not negatively affected but instead promoted to more vigorous levels. Such dual functions of the MEBO regenerative nutrients could explain why the MEBO regenerative nutrients exhibit little toxicity yet possess efficacy in suppressing tumor growth in animal models and clinically.
Recently, it has been recognized that mitochondria play new critical roles in cell metabolism ― regulation of cell death pathways. Gogvadze et al. (2008) “Mitochondria in cancer cells: what is so special about them?” Trends in Cell Biol. 18:165-173. Wang (2008) “The expanding role of mitochondria in apoptosis” Genes & Dev. 15:2922-2933. It has been reported that several mitochondrial proteins that reside in the intermemebrane space of mitochondria, in response to a variety of apoptotic stimuli, are released to the cytosol and/or the nucleus, thereby directly activating cellular apoptotic program and causing apoptosis of the cell. Liu et al. (1996) “ Induction of apoptosis program in cell-free extracts: requirement for dATP and cytochrome c” Cell 86:147-157. Verhagen et al. “Identification of DIABLO, a mammalian protein that promotes apoptosis by binding to and antagonizing IAP proteins” Cell 102:43-53. Based on our EM data obtained, the cancer cell death induced by the MEBO nutrients can be attributed to activation through disruption of mitochondrial membrane and subsequent releasing of the apoptotic proteins. In contrast, normal cells in the presence of the MEBO nutrients not only survive but also grow rigorously.
A number of agents, including chemotherapeutic drugs (e.g., cisplatin and arsenic oxide) and compounds isolated from natural sources (e.g., epigallocatechin gallate (EGCG) and beta-carotene) are shown to be able directly or indirectly target mitochondria, the “power plants” of the cell. Pederson (2007) “The cancer cell’s “power plants” as promising therapeutic targets: An overview” J. Bioenerg. Biomembr. 39: 1-12. However, there has been no report of these agents having a dual function of killing cancer cells while promoting normal cell growth and regeneration, as demonstrated by the MEBO nutrients. It is well known that virtually all of anti-cancer chemotherapeutic agents can cause the side effects of suppressing the growth of normal, fast dividing cells, such as epithelial cells in the skin, hair follicles and mucosa, as well as that of the hematological cells.
It is plausible that the intrinsic differences in the metabolism of normal and cancer cells may contribute to the differential response to the MEBO nutrients. It has been observed that cancer cells produce most of their ATP through glycolysis, even under aerobic conditions, and there is a correlation between glycolytic ATP production and aggressiveness of the tumor cells. Warburg (1930) “The metabolism of tumors” London: Arnold Constable. Simonnet et al. (2002) “Low mitochondrial respiratory chain content correlates with tumor aggressiveness in renal cell carcinoma” Carcinogenesis 23:759-768. When rapidly growing tumors shift their ATP production to glycolysis, mitochondrial activity slows down. Gogvadze et al. (2008), supra. By absorbing the highly lipophilic MEBO nutrients, the cancer cells seem to be unable to metabolize them; instead, the undigested lipid droplets stayed inside the cytoplasm, which caused swelling of mitochondria, leading to cell death (Figure 10.4.2c). In contrast, in the normal cell the nutrient droplets were taken into the cytoplasm and gradually metabolized by the cell (Figures 10.4.2d-e); mitochondria in the normal cells did not appear to be damaged by the uptake of the nutrients and continued to function normally, if not more vigorously. As demonstrated in the skin and mucosal tissue regeneration of wound and ulcer patients, the MEBO nutrients consistently promote physiological repair and regeneration of normal cells in humans, including fully developed adult humans.
The unique ability of the MEBO nutrients to promote normal cell growth without damaging the cellular power plants―mitochondria (as demonstrated in their clinical efficacy in promoting tissue and organ regeneration and in in vitro cellular studies) and their surprising ability to induce apoptosis of transformed and cancer cells are extremely desirable in the development of safe and efficacious products for cancer treatment and prevention. As MEBO nutrients are formulated using natural botanicals safely used for human consumption for thousands of years, these products have superior safety profiles and can be safely used a nutritional support for cancer patients, which forms the scientific foundation for MEBO’s ongoing large population human studies of end-stage cancer patients. See Section 10.10 below. This innovative approach to cancer treatment and prevention will open a new fertile field for basic and clinical applications.
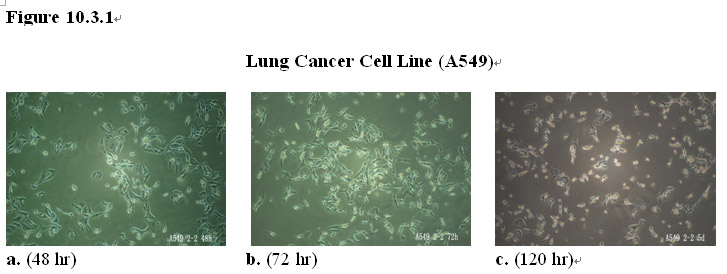
To further confirm the dual functions of the MEBO regenerative nutrients and selective cell-killing effects on human cancer cells, in vitro experiments were conducted in separate cultures containing A549 lung cancer cells (Figures 10.3.1a-c) and MRC5 normal lung fibroblasts (Figures 10.3.1d-f), respectively. The MEBO regenerative nutrients were added to both cultures.
After 48 hours of exposure to the MEBO regenerative nutrients, lung cancer cells manifested growth arrest and some cells showing morphology of cell death (Figure 10.3.1a). After prolonged exposure (>72 hours) virtually all cancer cells died in the culture (Figures 10.3.1b-c).
In contrast, in the presence of the MEBO regenerative nutrients normal lung fibroblasts proliferated vigorously and continued to do so to reach confluency by day 5 (Figures 10.3.1d-f).
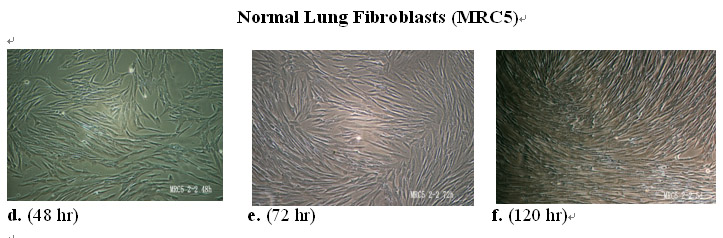
To test the effects of the MEBO regenerative nutrients on normal cells in the presence of cancer cells, in vitro co-culture experiments were conducted in a culture containing both normal bone marrow cells (small cells) and human gastric cancer cells (larger cells).
The co-culture was grown in normal culture medium (Figure 10.2.1a) and then divided into two groups: a treatment group and a control group. The MEBO regenerative nutrients were added to the co-culture in treatment group while the co-culture in the control group was maintained without adding any supplemental materials. As shown in Figure 10.2.1b, after 4 days of exposure to the MEBO regenerative nutrients, the cancer cells in the treatment group not only stopped growing but also manifested morphology of cell death. However, normal bone marrow cells in the treatment group not only survived but also proliferated vigorously. By day 7 virtually all cancer cells disappeared in the culture while the normal cells continued to proliferate (Figure 10.2.1c).
In comparison, in the absence of the MEBO nutrients by day 5 the cancer cells in the control group proliferated vigorously while the normal cells virtually disappeared in the culture (Figure 10.2.1d). By day 7, the cancer cells proliferated to reach confluency while no normal cells could be observed in the culture (Figure 10.2.1e).
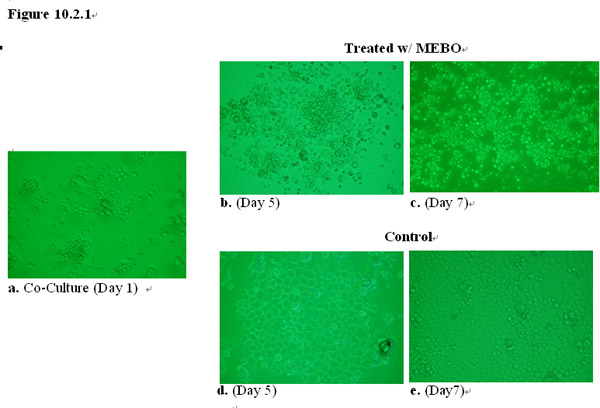
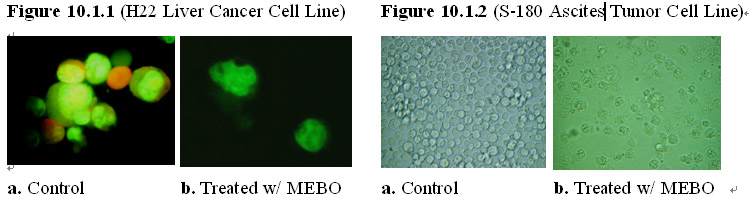
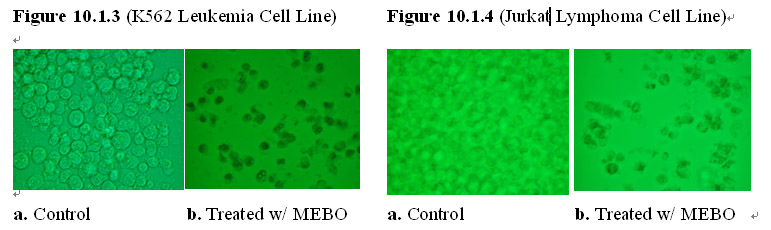
To test the effects of the MEBO regenerative nutrients on cancer cells, in vitro experiments were conducted in cultures containing typical cancer cell lines, including solid tumor cell lines, lymphoma and leukemia cell lines.
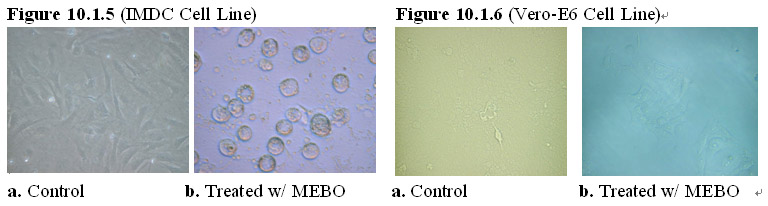
Typically, cancer cell lines were grown in normal culture medium and each cell line is divided into two groups: a treatment group and a control group. The MEBO regenerative nutrients were added to the cancer cell cultures in the treatment group while the cancer cell cultures in the control group were maintained without adding any supplemental materials. As shown in Figures 10.1.1-4, after 24 hours of exposure to the MEBO regenerative nutrients, solid tumor as well as leukemia cells in the treatment group manifested growth arrest with some cells showing the morphology of cell death. In comparison, the cancer cells in the control group proliferated at a normal rate and demonstrated normal cancer cell morphology. Prolonged exposure of the cancer cells (>48 hours) to the MEBO regenerative nutrients led to death of all cancer cells in the treatment group.
Interestingly, the MEBO regenerative nutrients also exert the same growth-arrest and cell-killing effects on transformed cells, such as an immortalized artery endothelial cell line (IMDC) and an immortalized kidney epithelial cell line (Vero-E6). As shown in Figures 10.1.5-6, after 24 hours of exposure to the MEBO regenerative nutrients, the transformed cells in the treatment group manifested growth arrest with some cells showing the morphology of cell death. In comparison, the transformed cells in the control group proliferated at a normal rate and demonstrated normal transformed cell morphology. Prolonged exposure of the transformed cells (>48 hours) to the MEBO regenerative nutrients led to death of all transformed cells in the treatment group.